We have a drug epidemic, but drugs are not an escape. Along with this epidemic there have been thousands of lethal overdoses. I like to review why so many people use street drugs or prescription pain pills. It started years ago with heroin injections had become more popular. But then heroin was getting a bad name, it became illegal, and prescription pain pills replaced heroin. Percocet, OxyContin and morphine prescriptions took off. Together with it the number of people with addiction increased drastically. The latest fashion craze is Fentanyl. Fentanyl works faster than morphine, but also wears off faster. One of the deadly side effects is respiratory depression. This means that a person cannot breathe and as a result will die. This is what is happening right now and what creates the news headlines.
Pain receptors
There are pain receptors all over the body, in muscles, organs and the skin. They are called nociceptors. Many medical conditions lead to pain in various parts of the body. For instance, with end stage degenerative arthritis bone rubs on bone. This causes a lot of pain in joints like the knees or the hips. Physicians often prescribe narcotics like OxyContin to control the pain. It may help for some time. But after a few weeks patients complain that the strength of OxyContin has worn off. The same dosage that gave them relief from the pain initially just does not give them relief any more. This observation is crucial. It is exactly what people who use OxyContin as illicit street drug found as well. The drug wears off, because the opioid receptors are getting weaker.
Pain receptor resistance
Nociceptors or opioid receptors are pain receptors. These receptors report pain to the body, and they have connections through the spinal cord to the brain. When an opioid is interacting with the pain receptor it inhibits acute pain to a large extent. But when the pain becomes chronic, the pain receptor is not working as well. More and more of the pain medication is necessary to achieve pain relief. Eventually the opioid medication is not working to relieve pain any more. The name for this phenomenon is “pain receptor resistance”. Scientific work behind why pain receptors get lazy in responding to opioids is still ongoing. In the meantime it simply is an observation. This is the reason why drug addicts are tending to increase the dosage of OxyContin or of Fentanyl. The toxic threshold of Fentanyl that is exceeded in the process is the reason for the deaths.
Insulin resistance
You may have heard of insulin resistance in diabetics. This is a very similar problem. With insulin resistance the diabetic no longer has a 100% response to insulin. This means that blood sugar is not going through cell membranes effectively as it should when the insulin receptor is working. The blood sugar values stay high and make the diabetes worse.
With pain receptor resistance the opioid is not giving the relief from pain it used to give. No wonder that the patient is feeling frustrated that the pain medication is no longer working properly.
Therapeutic index
The layperson does not normally know that there is a dosage for any drug where it becomes toxic. There is also a lower dosage where the drug is becoming effective. The difference between the two dosages is the “therapeutic window” or the “therapeutic index”.
Morphine has a therapeutic index of 70:1. Compare that to alcohol with a therapeutic index of only 10:1. Fentanyl has a therapeutic index of 300:1.
The danger of Fentanyl
One would think that Fentanyl should be safer than morphine, because the therapeutic index is larger. But the onset of Fentanyl is much faster than that of morphine and by the time drug users take Fentanyl they often are desperate for the drug to take their pain away and they overdose, which causes respiratory depression. If they are not intubated by an anesthetist and connected to artificial respiration, they die very quickly. Janssen Pharmaceutica first developed Fentanyl in 1959. Fentanyl was strictly part of the pre-anesthetic medicine for patients before going into surgery requiring a general anesthetic. The anesthetist was right there and would intubate the patient. That’s why we never heard of deaths from Fentanyl in the past.
If a person gets no pain relief from any opioid because of receptor resistance, the tendency is to increase the dosage. But this is what pushes the person into toxic ranges and this is what causes death from inadvertently suppressing the ability to breathe. People can get into trouble with alcohol overdoses, but the ordinary person usually knows how to handle alcohol. Fentanyl is a lot different due to the fact that respiratory depression (not being able to breathe) is one of the early symptoms that hits you suddenly.
What drugs do to your brain
Dr. Daniel Amen, a psychiatrist and brain researcher has used SPECT brain scans to produce images of different clinical conditions. This link shows the effect of a stroke, of Alzheimer’s disease and of drug abuse on the brain. Dr. Amen says that a brain can be rehabilitated. He has other SPECT images showing the images of an addicted brain and that of a rehabilitated brain. Spect scans are expensive. But they may be worth it, to impress a drug addict to stop the drugs and get rehabilitated.
Big Pharma and opioid drugs
In 1995 the FDA approved the use of OxyContin for chronic pain. Perdue Pharma, the drug company that had developed this opioid convinced the FDA that OxyContin stayed in the blood for 12 hours and they claimed that by being active longer than other opioids this would lead to better pain control and less addiction. It turns out that this was a slick sales pitch, however it was not true. Pain receptor resistance is as much a problem with OxyContin as with any other opioid. And the drug is as addictive as all the others. But the problem is that the FDA had approved OxyContin. What’s more, Purdue Pharma sent aggressive drug representatives to all the practicing physicians misleading them as well as the FDA that OxyContin would not be as addictive as other opioids.
Penalty for misrepresentation of OxyContin
In 2007 Purdue Pharma had to pay a fine of 634 million $ for misrepresenting the addiction potential of OxyContin. But the drug company was allowed to continue to market OxyContin. Since 2015 Purdue Pharma has been cashing in 2.4 billion $ annually from the sales of opioids including OxyContin. In the meantime Fentanyl, despite its danger of suppressing the ability to breathe, has taken off with regard to sales. Fentanyl also has taken over in terms of causing deaths across the US and other countries.
Alternative treatment of pain
According to Ref. 1 chances are that 70% of patients with back pain will get better with a few visits to an acupuncturist. In 1972 Dr. Ulett’s laboratory at the University of Missouri succeeded in getting the first NIH research grant for the study of acupuncture in the US. During these studies they found remarkable facts, the most important perhaps that electrical stimulation of acupuncture needles resulted in a doubling of the effectiveness of traditional Chinese acupuncture. After extensive research Dr. Ulett stated: ”The ancient practice of traditional Chinese acupuncture is now obsolete” (Ref.1). in the meantime the more effective electro-acupuncture has replaced acupuncture needles with the use of electrical skin pads.”
Other applications for electroacupuncture
Beside pain relief many other applications exist for electro-acupuncture. Addiction medicine makes use of electro-acupuncture in weaning people from morphine or heroine etc. It is effective to treat psychiatric illness, particularly depression. It is useful in relieving nausea and vomiting due to chemotherapy with cancer treatments or associated with pregnancy without affecting the pregnancy.
Prolotherapy
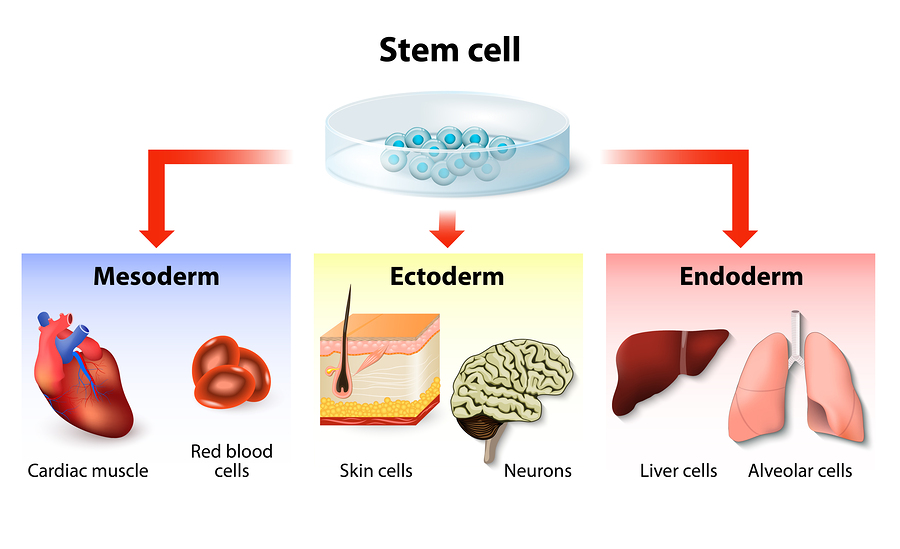
Prolotherapy has been successful for the treatment of back and neck pain, for arthritic pain and pain from chronic muscle spasm. When prolotherapy is done by itself 12.5% Dextrose is injected into the area of injury. Dr. Fields said that the reason it works is that there is activation of local stem cells in the injured area in the area of the Dextrose injection site. These stem cells will do the healing (details explained in an interview with Dr. Reeves). Further improvement of this technique and better results are possible by injecting a small amount of platelet rich plasma (PRP) very focally to an area of ligament rupture. PRP is obtained by centrifuging blood from the patient’s vein. The red blood cells are not necessary, but the platelet fraction and some of the plasma are part of the the PRP preparation.
It is often striking how much pain control occurs after only one or two prolotherapy treatments.
Stem cell therapy with PRP and low-dose laser therapy
This is a more direct way to get stem cells where the doctor wants them to do their work. Stem cell therapy with PRP and low-dose laser activation is the latest in terms of controlling pain. At the 22nd Annual Anti-Aging Conference in Las Vegas (Dec.10 to 14, 2014) Dr. Purita gave an overview of this method of pain control. He discussed the importance of the proper harvesting of PRP. He explained that apart from white blood cells (WBC) and platelets an important component of PRP are very small embryonic like stem cells (VSELs). They are visible through the microscope. The missing link has been the observation that white blood cells produce inflammatory substances, which have been detrimental in stem cell injections with PRP in the past. There was a poor survival rate of stem cells.
Low dose laser activation of stem cells and PRP
Photo-activation of the PRP before injection leads to anti-inflammatory behavior of the WBC in PRP. Dr. Purita calls this “light activated PRP”, which leads to the best results with stem cell/PRP injections.
Soft laser stimulation with red, green and blue soft lasers have also been effective to improve tissue healing significantly when stem cells and PRP are used together with light activation. The main sources for good stem cells are the fat tissue (from the “love handles”) and the bone marrow (obtained from pelvic bone). The stem cells mesenchymal stem cells (from fatty tissue) and bone marrow stem cells. The mix of all of this can mend osteoarthritic joints, degenerative disc of the spine, in short all musculoskeletal injuries that may be painful. The hallmark of healing with stem cells is that chronic pain disappears.
Curative treatment versus symptomatic treatment
It is one thing to treat a patient for pain symptomatically by prescribing OxyContin or other opioids. It is a completely other thing when the physician cures the pain by one of these alternative methods. Let us assume that a patient has a fall of a few step from a ladder and sustains a contusion of the lower back. This can be painful and may require a few pain pills. But if it does not improve within one week and diagnostic tests show that there is no fracture, electroacupuncture may be the solution to treat the pain rather than the use of an opioid. If this does not help, consider the combination stem cell/PRP/low-dose laser therapy. Chances are better than 80% that this will help. The patient will no longer suffer of pain. With healing life can go on: no pain pills. No addiction. No death.

Drugs Are Not An Escape
Conclusion
Conventional medicine treats pain symptomatically instead of treating the cause. It gets the physician to prescribe opioids, which can be the beginning of a series of tragic events. It can lead to drug addiction, dose acceleration, toxic effects of opioids including possible death through asphyxiation from no longer being able to breathe.
Stem cell therapy
The physician who concentrates on treating causes will use alternative methods to treat pain. The most effective of these methods is stem cell therapy. It is a mixture of adipose mesenchymal stem cells with bone marrow stem cells that are part of the therapy. The addition of platelet rich plasma is another part of the mix, and the final step is activation of stem cells with low-dose laser therapy. The cell mix is injected in the critical area. The end result is that the patient’s pain disappears, and it leads to a cure. The only situation where short-term opioids are justifiable is following surgical procedures. But even in these cases the narcotics should only be necessary for a few days to avoid serious side effects.
Reference 1: George A. Ulett, M.D., Ph.D. and SongPing Han, B.M., Ph.D.: “The Biology of Acupuncture”, copyright 2002, Warren H. Green Inc., Saint Louis, Missouri, 63132 USA
More info about electroacupuncture: https://www.askdrray.com/electro-acupuncture-twice-as-effective-as-conventional-acupuncture/
More about prolotherapy stem cell therapy: https://www.askdrray.com/prolotherapy-and-stem-cell-therapy/