Introduction
March is colorectal cancer awareness month, so let’s discuss prevention. Only 40 years ago cancer of the cervix was one of the major killers for women, but with the introduction of the Pap test this has all changed. For those women who get that screening done, there is no need for fear. The mortality rate from cervical cancer since the 1970’s has steadily decreased as shown in this link.
As far as cancer of the prostate is concerned, a lot of progress with regard to early detection has been made due to the introduction of the PSA blood test, which is used as a method of screening. As a result men are diagnosed earlier with prostate cancer resulting in more cures as the cancer found is at an earlier stage. Here is a link depicting the effect of the PSA test on mortality rates from prostate cancer in time.
March is colorectal cancer awareness month, so let’s discuss prevention
March is colorectal cancer awareness month as this article explains. The key is early detection and treatment as with any type of cancer. Specifically, with rectal and colon cancer there are mostly no symptoms, as blood in stool or any other symptoms occur only late into the disease. What we do know, however, is that there is a long latent phase where precancerous mucous membrane changes lead to polyps and these will degenerate in time into cancer of the colon or rectum.
Not everyone has the same risk of developing colon cancer or rectal cancer. There are people with a higher rate of colorectal cancer, as they carry a susceptibility gene in their families. A healthy lifestyle can also reduce the risk of colorectal cancer.
March Is Colorectal Cancer Awareness Month, So Let’s Discuss Prevention
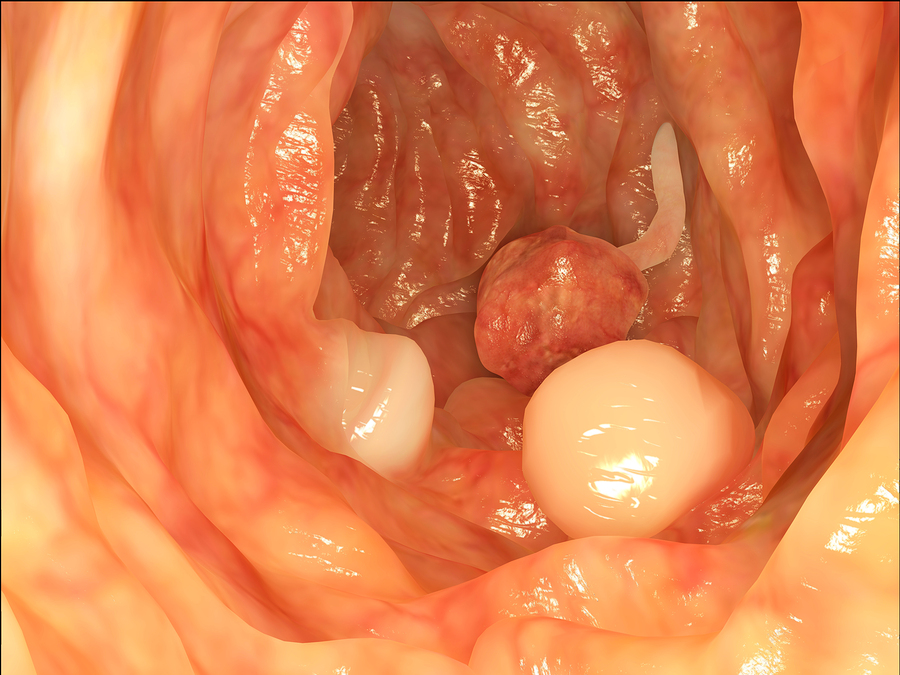
Polyps are the precancerous precursors for colorectal cancer
It is now widely accepted that polyps are the precancerous precursors for colorectal cancer and colonoscopies done on everybody starting at age 50 (those with family risk factors much earlier) have already been shown to have decreased the frequency of the disease as the data from the CDC show. The problem is that the survival curves for colorectal cancer have only a swallow incline. A steeper decline would mean better survival of colorectal cancer patients. In the case of the mortality rates of cervical cancer and prostate cancer the slope showed a more rapid decline translating int much better survival rates.
Not enough colonoscopies are done
The incidence of colon cancer should have gone down to almost the zero point. All that has been achieved so far is a reduction of a portion of cases (those who went for colonoscopies early enough before it turned into colon cancer); this is by far not an elimination of colorectal cancer. The reason for this is the fact that in many cases people have colonoscopies too late when the polyp has already turned cancerous, or invasive colon or rectal cancer is already present at the time of the first colonoscopy.
Designating March as colorectal awareness month makes a lot of sense to me
I happen to come from a family where my mother died in 1980 from colon cancer at the age of 59. Because of this my doctor told me that I have a risk of about 3-fold higher than the population at large to also develop colon cancer. I have had colonoscopies since the age of 40 every 3 years. Ironically a few days ago right during the colorectal awareness month, I was getting my 9th colonoscopy. On three occasions polyps were removed, which tells me that the cancer-screening program works!
Why screen for colon cancer in regular intervals?
So why is it important to screen in regular intervals? One reason is that we are now exposed to more toxic chemicals in our environment and food than 100 years ago. So all cancers, but especially colorectal cancer rates have increased. We know the pathophysiology, which is the science that studies how an illness develops. We know that it takes several years between the occurrence of the first precancerous cells that form in the lining of the gut (called “mucosa”) and the formation of polyps. It takes another few years before polyps turn cancerous. This means that there is enough of a time interval to do screening. If we are not aware of this and ignore it (as unfortunately many people do), the process will run down the conveyor belt on an automatic program, which ends up in end stage colorectal cancer. The stages of colon cancer are depicted in this link.
Invasive colon cancer is deadly
As the table of my chapter on colon cancer staging shows, the invasive end stage colon cancer (stage IV or Duke D) has a 5-year survival rate of only 6%. Even when the cancer is limited to stage II (also called Duke stage B) there would be a 5-year survival of only 80% (see table in link).
What does screening really achieve? On an individual basis the gastroenterologist who does the colonoscopy can screen the whole colon for premalignant polyps and remove them during the procedure. This moves the potential cancer staging backwards to beyond any detectable cancer, as all of the potential early cancer cells would have been inside the polyp (called local “in situ” disease) and were removed by cauterizing the stalk (see above link). There is another potential factor that can help to reduce colorectal cancer incidence: Recently a connection was made between
Helicobacter pylori as a risk factor for colorectal cancer
Helicobacter pylori (H. pylori) infection of the stomach and polyps in the colon as well as colon cancer. In the past several smaller studies failed to show this correlation. It took 156,269 patients in this study to show that there was a correlation. As H. pylori is being tested for and treated more and more, this will also have a positive effect on lowering the frequency of colorectal cancer.
Mass colonoscopy screening
On a population basis with mass colonoscopy screening the incidence of colorectal cancer is reduced. The reduction of colon cancer would be much faster. Eventually it would turn into a disease similar to cancer of the cervix. Here it still matters whether you screen or not, but very few people have to suffer from it. Here is an image from a paper (look for Fig. 2, halfway down the page). It shows that survival benefits (longer lives) are registered only after 10 years or more following colonoscopy.
Colorectal cancer statistics
Every polyp that is removed will add up to the colon and rectum health of the nation at large. This shows statistically, when you sum up all of the colonoscopies done around the country year after year. We need a nationwide and worldwide awareness that colorectal cancer screening is something worthwhile doing. This cancer is the third most frequent cancer in many parts of the world.
I am grateful that colonoscopy screening works, as I had polyps removed three times over a 29 year span and I did not have to go through all the surgical procedures that my mother had to endure. Had I lived 50 years earlier I may not have lived long enough to tell you how important colonoscopy screening is.
Here are the recommendations
-
-
- Let us assume there is no risk of colorectal cancer in your family. In this case screen once at the age of 50. This makes sure you are not one of the spontaneous colorectal polyp producers. If OK, screen every 10 years provided the colonoscopy is always negative.
- A family history of direct bloodline relative increases the risk for colorectal cancer. Direct bloodline relatives are: mother, father, brother or sister. If one of them had cancer of the colon or rectum, you have a higher cancer risk. In these individuals a gastroenterologist must do colonoscopies every 3 years.
-
Missed polyps during a colonoscopy
-
-
- There may be up to 15% of missed polyps during a colonoscopy. But with the next colonoscopy there is a high likelihood that the physician catches the abnormal polyp in time. The pathologist confirms that the subsequent screening caught them before they turn cancerous.
- There are special cases, families with genetic syndromes like the familial polyposis of the colon. In these families a gastroenterologist needs to screen children/young adults for polyps when they are still young. This is from the age of 20 to 25 years onwards.
-
Don’t complain, if you belong to category 1 or 2 as it could be much worse (category 3). Cancer is serious business. Remember, March is colorectal cancer awareness month.
More information about colon cancer.




