There was an interesting workshop alongside of the A4M conference mid December 2014 organized by Jonathan Schwartz who gave an overview of the use of low-dose laser therapy for various clinical applications. It involved the use of the Dr. Michael Weber low-dose laser machine, which has a lot of versatility.
- First there are 5 laser light frequencies in the rainbow colors (infrared, red, yellow, green, blue) and the colors have very special characteristics as will be explained further below.
- There are a multitude of applicators like skin acupressure point applicators, a shower for hair loss applications, a head adapter, which looks like a crown. With this device red light will penetrate into the brain through the skull bone. There is also a mouth shower and various lengths needle applicators that can be used to access the body intravenously or interstitially (direct tissue approach). At the center of the equipment is the Weberneedle Compactlaser, which can be attached to the various applicators.
Laser characteristics
The blue laser penetrates about 1 cm (0.39 inch) under the skin, a green laser penetrates only 0.5 cm (0.19 inch); like the blue laser the yellow laser penetrates through the skin with a depth of 1 cm (0.39 inch). The red laser has a penetration depth of 2-3 cm (a bit more or less than 1 inch) and the infrared laser penetrates 5-7 cm (2 to 2 1/2 inches).
In addition the various lasers have different inherent qualities: The red laser is good for tissue regeneration, which lends itself for chronic pain. Green and blue lasers have anti-inflammatory effects, which helps in acute pain. The yellow laser can be used for detoxification, has antidepressant qualities and photosensitizes hypericin, a substance derived from St. John’s wort, which is known to have antidepressant qualities. The various types of laser mentioned can be used interstitially, intravenously and just on the skin surface over acupuncture points. Dr. Weber explained that detailed research has revealed that the low-dose energy beam sends out energy that is taken up by the surrounding tissues and cells. The mitochondria of the cells get activated to produce more ATP, which the cells use to heal themselves.
Meeting in Placentia
Forward to a meeting in Placentia, CA on Feb. 7, 2015 where Dr. Michael Weber and several other speakers gave presentations on the use of the Dr. Weber laser system. A number of local doctors who had an interest in learning more about the low-dose laser system were there as well. It was a daylong mini conference.
Three volunteers were used to demonstrate the use of the system. I was volunteering about a chronic left lower back pain that various chiropractors had problems adjusting in the past year. I have a strong family history of arthritis on my mother’s side and my maternal grandmother’s side as well. The health professionals thought that I likely have developed arthritis in the left sacro-iliac joint. Dr. Weber used the interstitial needle, which is 4 cm (1.57 inches) long. The skin was injected with a local anesthetic first, and then the needle was inserted, which I could hardly feel. Now he injected 5 cc of normal saline. This was used, so that the laser light would spreads more into the surrounding area. Dr. Weber explained that he was very close to the SI joint with the tip of the needle on the left. He attached a blue laser to it for 20 minutes and switched it to a green laser for another 20 minutes.
In the meantime the other two volunteers were treated.
One was a physician in the group who had a chronic planter’s fasciitis. He was treated with an intravenous laser application. First a special butterfly was inserted, through which a sterile laser probe could be threaded and then attached. He received a red laser.
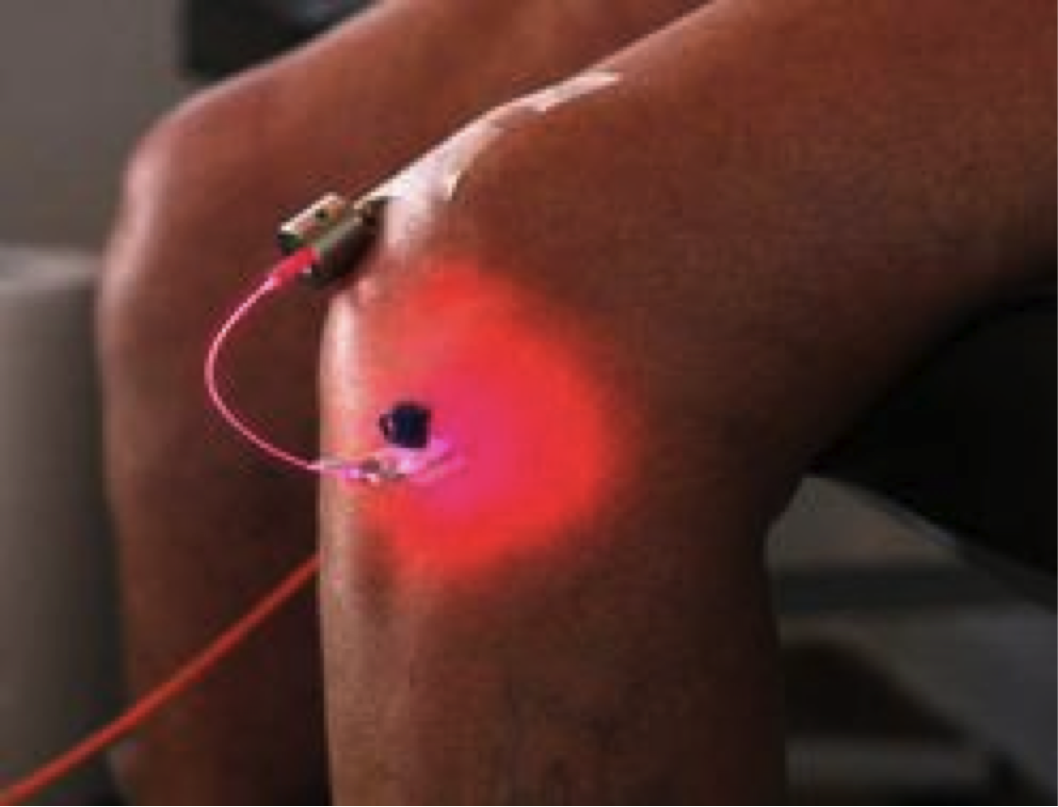
The third volunteer had a chronic right knee problem from congenital Osgood Schlatter disease. In him Dr. Weber used an approach of intraarticular injection and he attached a blue laser for 20 minutes, followed by a yellow laser for another 20 minutes. A physician with a California license supervised all of these procedures.
I woke up the following day with no pain in my left lower back, but at the same time the lesser right lower back pain had also disappeared. I figure that due to the fact that my back mobility is back the untreated right side must have normalized as well. It is now 7 days following the procedure and I still have no back pain. Yesterday I saw my local chiropractor in Southern California and he confirmed that my back was much easier to adjust than the month before (Update April 12, 2015: my lower back is still pain free!).
Normally a case like mine would require 5 to 6 weekly treatments before the problem is resolved. Dr. Weber explained that more complicated problems like fibromyalgia would take 15 to 20 treatments in succession or more. The principal is always that you treat where the symptoms are; in the follow-up visit the healthcare practitioner treats the remaining symptoms until all of the symptoms have resolved.
The intriguing fact is that low-dose laser therapy seems to fit right into gap where conventional medicine has failed.
Clinical cases that respond to laser therapy
Dr. Weber has collected clinical cases that improve with laser treatments, such as diabetes, chronic liver diseases, chronic pain syndromes, rheumatoid arthritis, polyneuropathy, chronic inflammatory disease, cancer (with photodynamic therapy), fibromyalgia, high blood pressure, ringing in the ears (tinnitus), macular degeneration, multiple sclerosis, chronic fatigue syndrome, Lyme disease, allergies and eczema. This, however, is just a partial list.
Photodynamic cancer therapy is made possible by the fact that certain substances have absorption spectra that are activated by different wavelength. This amplifies the effect of the natural substance that is used by several folds. For instance Chlorin E6 absorbs a red laser (around 660 nm). A blue laser activates Curcumin. A yellow laser activates Hypericin. Here is a website that explains the principle of phototherapy.
Various cancers can be treated where conventional medicine has so far failed. Examples are lymph metastases from breast cancer, pancreatic cancer, and bladder cancer. I have blogged regarding a combination treatment for breast cancer before, where phototherapy with lasers and immunostimulation were combined. Esophageal cancer is treated through esophagoscopy combined with a laser that activates curcumin, which had been taken orally well before the procedure. Not all of the cases are successful, but the majority of them are.
Otherwise routine low-dose laser applications are used for tendinitis, tennis elbow, sprains and soft tissue injures.
Laser-Therapy-Going-Beyond-Skin-Deep
You can combine the laser system with prolotherapy. Prolotherapy is done first by injecting hyperosmolar dextrose solution, which is a strong stimulator of stem cells. Using the same needle, but attaching the Weber low-level laser therapy will activate the stem cells and protect them from dying off.
Conclusion
Low dose laser therapy using the Weber Medical technology is a new treatment modality available to the interested physician. I think that it will cause a revolution within medicine. It is scientifically sound and it fits right into the difficult to treat patients; the patients that otherwise would be unlikely to respond. However, they will respond well to these new treatment modalities. Apart from musculoskeletal problems, various cancers will also respond to this. The Mayo clinic is starting a study on treating cancer using phototherapy and the Dr. Weber low-dose laser system.






