We have been exposed to a lot of clichés about aging, which makes it more difficult to dispel rumors and to clearly focus on what can and what cannot postpone aging and the associated disabilities. Here I will attempt to summarize what is known about this topic.
The American Academy of Anti-Aging Medicine (also known as A4M) has published a book where all of this is discussed in detail (Ref.1). But there are yearly conferences as well in Las Vegas and other places where further details regarding anti-aging are discussed. Since 2009 I have been attending the conferences in Las Vegas regularly every year.
Based on this knowledge let me start by reviewing the tools of anti-aging that can be used to slow down the process of aging significantly.
- Mitochondria
At the center of anti-aging is the preservation and metabolic optimization of the mitochondria. Each of our cells contains little particles called mitochondria, which is where our energy metabolism takes place. Mitochondria function like mini-batteries.
The citric acid cycle builds up ATP, which is subsequently hydrolyzed into ADP and orthophosphate releasing energy for cell metabolism.
Old people who shuffle when they walk and have difficulties climbing stairs have lost significant amounts of mitochondria and simply run out of energy. The key to prevent this from happening is to preserve our mitochondria. We inherited them from our mother, because only the head of the sperm, which does not contain mitochondria entered the ovum when the egg cell that was destined to become you was fertilized. Subsequently the mitochondria from mother’s egg have provided all of the mitochondria in the cells of our body.
- Preserving mitochondria
There are supplements that specifically preserve mitochondria: PQQ (=Pyrroloquinoline quinone) helps mitochondria to multiply. A typical dose to take every day is 20 mg. Mitochondrial aging is slowed down by ubiquinol (=Co-Q-10, 400 mg per day is a dose that I recommend). Co-Q-10 repairs DNA damage to your mitochondria.
There are simple lifestyle changes that you can make: eat less calories as this will stimulate SIRT1 genes, which in turn stimulate your cell metabolism including the mitochondria.
Resveratrol, the supplement from red grape skin can also stimulate your mitochondria metabolism. 300 to 500 mg of trans-Resveratrol once daily is a good dose.
Build in regular exercise into your day – and I mean every day– as this will also stimulate your mitochondria to multiply similar to the effects of PQQ. Lipoic acid is an anti-oxidant that counters the slow-down of mitochondrial metabolism. I recommend 300 mg per day.
L-arginine is an amino acid that is a precursor of nitric oxide (NO). Red beet is a rich source of nitric oxide, which is directly released into your system. There are also commercial products for NO. This keeps the arteries open, prevents high blood pressure and also hardening of the arteries and has a direct effect on preserving mitochondria.
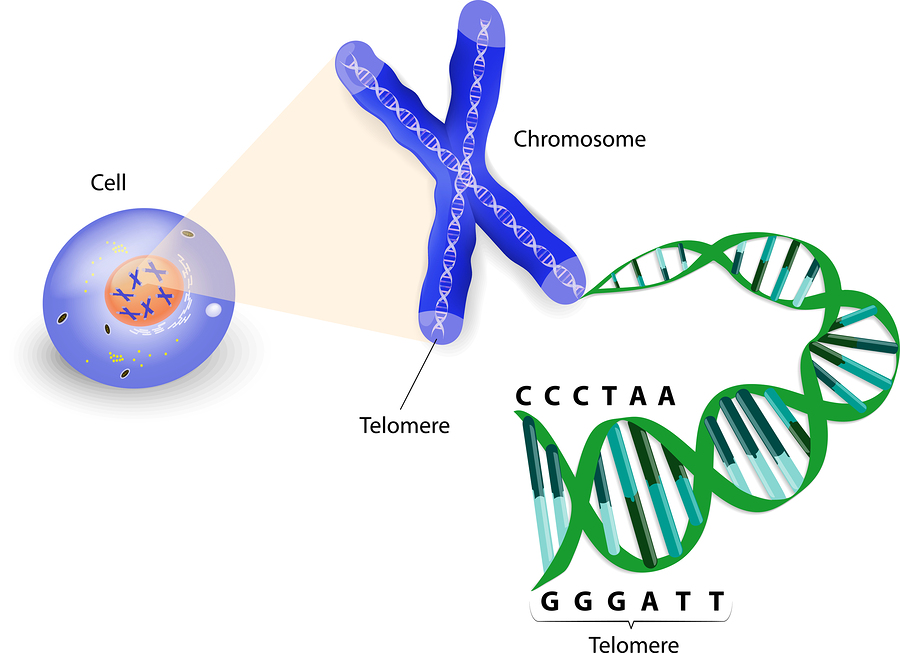
Researchers from the McKusick-Nathans Institute of Genetic Medicine of the Johns Hopkins University School of Medicine in Baltimore, MD found that mitochondrial DNA content varies according to age (less mitochondrial DNA in older age), sex (yes, women have more than men) and mitochondrial DNA; it even has an inverse relationship to frailty and a direct relationship to life expectancy. This paper was published in February of 2015.
Each mitochondrion has its own mitochondrial DNA contained in 2 to 10 small circular chromosomes that regulate the 37 genes necessary for normal mitochondrial function.
In multi ethnic groups it was apparent that mitochondrial DNA content was dictated by the age of a person.
Frailty was defined as a person who had aging symptoms including weakness, a lack of energy compared to the past, activity levels that were much lower than before and loss of weight. When persons with frailty as defined by these criteria were identified, they were found to have 9% less mitochondrial DNA than nonfrail study participants.
Another subgroup were white participants; when their bottom mitochondrial DNA content was compared to the top mitochondrial DNA content, the researchers found that frailty was 31% more common in the bottom DNA content group. This means that white people are more prone to frailty and they should take steps early on to prevent this from happening.
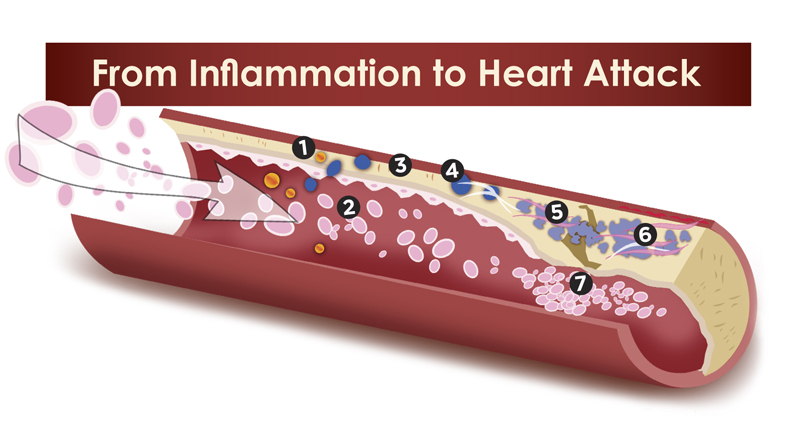
- Slowing down hardening of our arteries
It makes sense that young people who do not have signs of hardening of their arteries have better blood supply to their cells and thus supply their mitochondria with more oxygen and nutrients than frail, older people. The same is true for people who exercise regularly.
Vitamin D and vitamin K2 have been shown to lower calcium in the blood vessels and to retain calcium in the bone preventing osteoporosis. This is particularly useful in postmenopausal women. This October 2014 publication mentions that apart from vitamin D and vitamin K2 resveratrol and inositol are additional factors helping to prevent heart disease and osteoporosis.
This September 2013 publication confirms that a deficiency for vitamin K2 is common in the general population. This deficiency leads to osteoporosis and calcification of the arterial wall and causes heart attacks, strokes and bone fractures. Supplementation with vitamin K2 at 200 micrograms per day every day is recommended to prevent this from occurring.
- Sugar and starchy foods
You need to understand that starchy foods equal sugar, once digested. As a result a refined cereal breakfast=sugar, pasta=sugar, bread=sugar, donuts=sugar, potatoes=sugar and so on. It has to do with the glycemic load. When you cut out sugar and starchy foods (meaning that the glycemic index of the foods you eat is below 50) you will shed 30 to 50 pounds of weight within 3 to 5 months, if you are overweight or obese. You will feel a lot more energy. Your blood vessels will be cleaned out as the oxidized LDL cholesterol will disappear and the HDL cholesterol will mop up what cholesterol deposits were there before.
It is certainly good for you, if you are not into the sugar and candy stuff, but the seemingly harmless pizza and all the other starchy foods mentioned above are of concern as well. All of the high -glycemic carbs stimulate the pancreas to produce insulin. This in turn produces inflammation in tissues including the brain. Alzheimer’s disease is one of the complications of this.
Where does this leave us? For decades we have been told that saturated fats and cholesterol in our diet were the culprits and we replaced them with sugar that is part of a low-fat diet. We need to pay attention to the glycemic index and cut out high glycemic foods. However, it is OK to eat some carbs from the medium glycemic food list and most of our carbs from the low glycemic food list. With regard to fat it is important to consume only the healthy fats like olive oil, coconut oil and omega-3 fatty acids. As you make these adjustments to your life style you will also prevent many cancers, as you normalize the body’s metabolism and help prevent chronic inflammation, which can cause arthritis and cancer. Finally, pay attention to stress management. The body and the mind work together. Uncontrolled stress leads to heart attacks and strokes.
- Cut down on processed foods
Processed foods contain the wrong type of vegetable oils that are composed of omega-6 fatty acids. This disbalances the ratio of omega-6 fatty acid versus omega-3 fatty acids. This is typical for all the processed foods, but also fast food places in the industrialized world. The consequence of this disbalance is the formation of arachidonic acid and inflammation of tissues. This causes high blood pressure from inflammation of the arteries, arthritis from inflammation in the joints and can irritate the immune system to the point of causing autoimmune diseases. The end result after decades of exposure to a surplus of omega-6 fatty acids are disabilities from end stage arthritis, as well as heart attacks and strokes from inflammation of the arteries due to the hardening of the arteries.
The remedy for this is to cut out all processed food and stick to the basics of preparing your own food from healthy ingredients with no food preservatives.
Use olive oil for salads and coconut oil for cooking. Take omega-3 supplements to restore the omega-6/omega-3 fatty acid balance.
- Replace hormones with bioidentical ones
When I watch postmenopausal women, many look prematurely aged with sagging skin in their faces. Had they replaced their missing hormones when they entered menopause, the bioidentical hormones used for replacement therapy would have helped their skin to remain younger looking, hardening of the arteries would have been postponed and osteoporosis in the bones would also have been prevented.
With men it is now known that testosterone is vital for prevention of prostate cancer, but it is also important to prevent heart attacks, strokes and dementia as they age.
I would recommend that you see a naturopath or an anti-aging physician to have your hormones checked and if necessary start replacement with bioidentical hormones.

Ageless Aging
Conclusion
Slowing down aging and avoiding disabilities from aging are now a possibility, if we manage our lives in a way that the biochemistry of our bodies remains the same and our mitochondria continue to function, even when we get older. I discussed the details of how to do that above. I have also written a book on the subject of anti-aging, which deals with these topics in more detail.
I hope that you incorporate at least some of these steps in your life to prevent suffering from disabilities as you age and to avoid premature aging.
References:
Ref.1: Ronald Klatz, MD, DO and Robert Goldman, MD, PhD, DO, FAASP, Executive Editors: “Encyclopedia of Clinical Anti-Aging Medicine & Regenerative Biomedical Technologies”. American Academy of Anti-Aging Medicine, Chicago, IL, USA, 2012.