Dr. Nalini Chilkov gave a talk about how obesity and diabetes can cause cancer. The original title was “Integrative Cancer Care, Increased Rates of Cancer and Cancer Mortality Associated with Obesity and Insulin Resistance, Nutraceutical and Botanical Interventions”. She presented her talk at the 24th Annual World Congress on Anti-Aging Medicine (Dec. 9-11, 2016) in Las Vegas that I attended.
In the following I will present a brief summary of her lecture.
Obesity is a major risk factor for cancer
Obesity causes 14% of all cancer deaths in men and 20% of cancer deaths in women. This link explains this in more detail. The following 15 cancers related to obesity in terms of causation. They are: colon cancer, gastric cancer, gallbladder cancer, ovarian cancer, breast cancer, liver cancer, uterine cancer, endometrial cancer, rectal cancer, pancreatic cancer, cervical cancer, non-Hodgkin’s lymphoma, renal cancer, multiple myeloma and esophageal cancer.
The American Society of Clinical Oncology reported about a meta-analysis involving 82 studies. This involved more than 200,000 women with breast cancer. The researchers compared premenopausal and postmenopausal women who were obese or normal weight. Premenopausal, obese breast cancer women had a 75% increase in mortality compared to the normal weight breast cancer group. In comparison with the normal weight group the postmenopausal group of obese breast cancer women showed a 34% increase of mortality.
With obese prostate cancer patients there is a similar observation. Obese patients have a more aggressive prostate cancer on the Gleason score and the cancer is in a more advanced stage at the time of diagnosis.
Diabetes increases mortality from cancer
Obesity is a common risk factor for both cancer and diabetes. But diabetes by itself is also increasing mortality of several cancers. In a consensus report details of the relationship between cancer and diabetes have been discussed in detail. The following cancers have been identified to have an increased risk of diabetes: pancreatic, gastric, esophageal, colorectal, liver, gallbladder, breast, ovarian, endometrial, cervical, urinary bladder, renal, multiple myeloma and non-Hodgkin’s lymphoma.
A meta-analysis suggests that cancer patients who are diabetic have a 1.41-fold increased risk of dying compared to those cancer patients who have normal blood sugars. Dr. Chilkov explained in detail what the various mechanism are that account for the faster cancer growth in obese and diabetic patients. High insulin levels is one of the risk factors, so is IGF-1, an insulin-like growth factor. The aromatase enzyme in fatty tissue turns male type hormones into estrogen, which also can stimulate cancer growth.
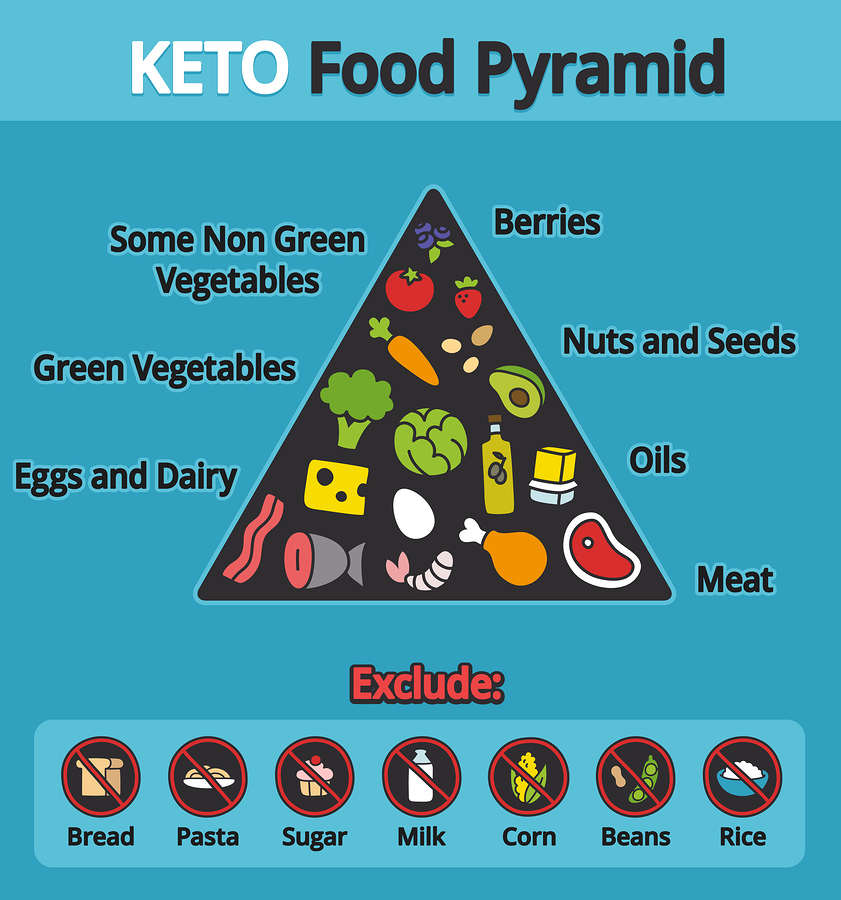
Carbohydrate restriction diet to prevent obesity
Low carb diets like the Mediterranean diet, the ketogenic diet and the Atkins diet will drop blood insulin and lactate levels. Cancer size and cancer growth are related to insulin and lactate levels. A low carb diet can reduce insulin-mediated uptake of sugar into cancer cells.
Research has shown that cancer metabolism slows down when a 10%-20% carb/high protein diet is consumed by the patient. This reduces the amount of sugar that is taken up by cancer cells. It also reduces insulin, so there is less cancer growth. A ketogenic diet is a more strict way to restrict carbohydrates. Intermittent fasting is also a useful method to reduce carbohydrate intake.
Here is an interesting study that illustrates the power of intermittent fasting. The study involved 2413 patients with early breast cancer who were followed for 7 years. Those breast cancer patients, who consistently did not eat anything between dinner and breakfast for 13 hours or more, had a 36% lower risk of having a cancer recurrence. There was also a 21% lower risk of dying from breast cancer when fasting was done for 13 hours or more overnight.
Supplements to prevent obesity, diabetes and cancer
A low carb diet and in some cases even a ketogenic diet is beneficial as a baseline. A regular exercise program is also useful for general fitness building and cardiovascular strengthening. In addition Dr. Chilkov recommended the following supplements.
- To reduce inflammation in the body, Dr. Chilkov recommended taking 2000 to 6000 mg of omega-3 fatty acids per day (molecularly distilled fish oil).
- Berberine 500 to 1000 mg three times daily. Dr. Chilkov said that Berberine has anti-cancer properties, improves insulin sensitivity and reduces absorption of sugars in the intestinal tract.
- Curcumin inhibits cancer cell division, invasion and metastatic spread through interaction with multiple cell signalling proteins. Several researchers showed that curcumin could lower blood sugar levels by stimulating insulin production from beta cells in the pancreas. Triglycerides, leptins and inflammation in fat cells are also lowered by curcumin. Insulin sensitivity increases through the action of curcumin. Dr. Chilkov recommended 300 mg/day of curcumin for 3 months.
- Resveratrol, the bioflavonoid from red wine is a powerful anti-inflammatory. This antioxidant has several other effects, which make it challenging to measure each effect by itself. This group of investigators managed to simultaneously measure these effects. They found that resveratrol lowered the C-reactive protein by 26% and tumor necrosis factor-alpha by 19.8%. Resveratrol also decreased fasting blood sugar and insulin; in addition it reduced hemoglobin A1C and insulin resistance. The recommended daily dose of resveratrol is 1000 to 5000 mg.
- Green tea catechins (EGCG) help to normalize the glucose and insulin metabolism. The dosage recommended was 1-3 grams per day.
- Reishi mushroom (Ganoderma lucidum) contain polysaccharides with antidiabetic and antiobesity effects. They make gut bacteria produce three types of short-chain fatty acids that control body weight and insulin sensitivity.

Obesity And Diabetes Can Cause Cancer
Conclusion
Obesity is a risk factor not only for diabetes, but also for cancer. Chronically elevated blood sugars, increased fasting insulin levels and increased IGF1 levels can cause cancer. In addition they can stimulate tumor growth and increase cancer mortality. It is for this reason that the health care provider should screen all diabetics for cancer. In her talk Dr. Nalini Chilkov gave clear guidelines what supplements will be beneficial to reduce the risk of obesity and diabetes as well as cancer. Start with a healthy, balanced diet. Add an exercise program. Then consider some of the above-mentioned supplements to reduce your risk for cancer, diabetes and obesity.