Several animal and human studies by the Mayo Clinic showed that removal of senescent cells can extend life. Researchers Xu et al. showed in 2018 that senescent cells weaken the body. Senescent cells are damaged cells that are still living. They can cause the release of inflammatory cytokines. The researchers showed in mouse experiments that intermittent senolytics increased life expectancy by 36%. Senolytics are drugs that dissolve senescent cells; the senolytic cocktail consisted of dasatinib plus quercetin.
In these mouse experiments their risk of dying was reduced by 65% compared to control mice that did not take senolytics.
Senescent cells causing premature aging
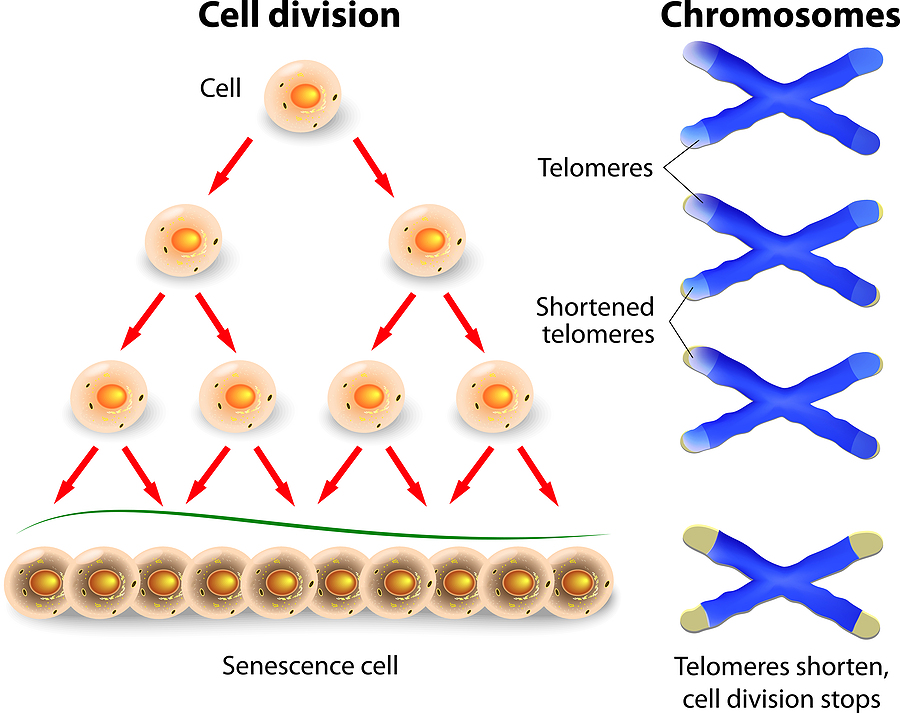
In the past 5 years research on aging and on chronic diseases made a lot of progress. Researchers realized that the accumulation of senescent cells is what causes both. All this happens because the process of apoptosis, the removal of dead cells, is impaired in the aging person. It appears that in older age there is a problem with dying cells and their removal. Instead they linger on and start producing cytokines, which cause inflammation. This can damage other cells and lead to organ failures. All this explains why older people often get chronic diseases and do not reach their normal lifespan. The accumulation of senescent cells also blocks regenerative factors that improve one’s health.
Senolytics
Dasatinib is a kinase inhibitor that was developed to treat acute myelogenous leukemia in adults and children. Researchers did animal experiments with a combination of dasatinib and quercetin for several years. They also have started smaller pilot clinical trials in humans. It appears that the human findings are very similar to the animal findings. But more research is needed to answer questions about side-effects and effects of removal of senescent cells.
Details about animal experiments with senolytics
The Mayo Clinic research showed that old mice treated with senolytics (dasatinib and quercetin) live 36% longer than controls that did not receive senolytics. Another part of this series of experiments showed that senescent cells are indeed what kills prematurely. They took senescent cells from old mice and transplanted them into young mice. Soon the young animals showed deterioration health wise and they died prematurely. Another control group were older mice that received senescent cells from old mice. They too died prematurely. Treatment with senolytics (dasatinib and quercetin) improved physical functioning and also survival.
Details about human trials regarding senolytics
For three days 11 participants received senolytics (dasatinib and quercetin). The effect of the drugs was evident for 11 days. The subjects took 100 mg of dasatinib daily and 500 mg of quercetin twice per day for 3 consecutive days. This dose was repeated twice more on a weekly basis for a total of 3 weeks. These patients had idiopathic pulmonary fibrosis. This is an incurable disease where senescent cells accumulate. These patients showed significantly improved gait speed, walking endurance, chair rise test performance and scores of other physical performances. All this occurred on day 5 after the initial dose of senolytics.
Alternative senolytics, so removal of senescent cells can extend life
Dasatinib as a senolytic has significant side effects.
For this reason, researchers looked for alternatives. Theaflavins, isolated from black tea fits this bill. It is non-toxic, but it is also effective as a senolytic. Researchers from Life Extension have developed a senolytic product containing theaflavins and quercetin. Instead of regular quercetin they included quercetin phytosome, which has 50-times more potent bioavailability. One capsule contains 74 mg of quercetin phytosome (the equivalent of 1250 mg of regular quercetin) and 275 mg of theaflavins.
Discussion
Future research needs to show whether or not the Life Extension senolytic indeed does what it promises. It claims that only one capsule per week stimulates apoptosis, reduces cytokines and increases longevity. I would like to see a clinical study that examines all these parameters. One measure of longevity is to determine the length of leukocyte telomeres. All the other laboratory tests are readily available. Research in this field will certainly continue and scientists will likely develop other senolytics.
Removal of Senescent Cells Can Extend Life
Conclusion
The accumulation of senescent cells causes both aging and chronic diseases. Research showed that in older age the process of apoptosis, the removal of dying cells, is incomplete. As a result dying cells accumulate. They produce inflammatory cytokines, can damage other healthy cells and lead to chronic organ failure. In addition, cancer cells can develop and the patients can die prematurely. Senolytics are substances that clear out senescent cells. In mouse experiments they have already led to improved survival and health. Clinicians performed a clinical trial on patients with idiopathic pulmonary fibrosis, which is an incurable disease where senescent cells accumulate. They showed significantly improved gait speed, walking endurance, chair rise test performance and scores of other physical performances. One pill once per week with dasatinib and quercetin can achieve this. More research in this area can clarify why senolytics work and what the side effects are.